Please click here to view the model.
Both concurrent chemoradiotherapy (CCRT) and induction chemotherapy (ICT) followed by CCRT are recommended for advanced nasopharyngeal carcinoma (NPC).
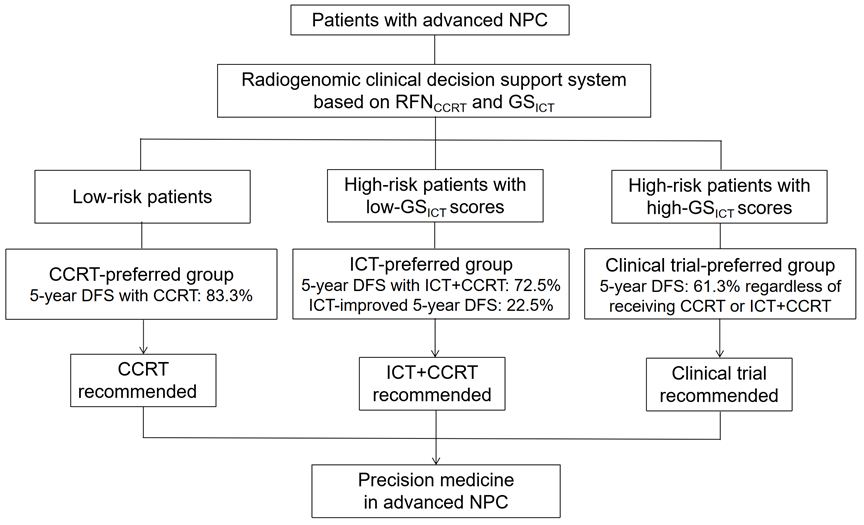
However, tailoring personalized treatment is still lacking in clinical practice. Here, we established a radiogenomic clinical decision support system to classify patients into three subgroups according to their predicted survival with CCRT and ICT response, which were optimal candidates for CCRT, ICT plus CCRT, and clinical trials, respectively.
This work paves the way for precision medicine in advanced NPC and has been published at iScience, titled “A radiogenomic clinical decision support system to inform individualized treatment in advanced nasopharyngeal carcinoma”.